Across the North Sea, the Kingdom of Norway with it’s Scandinavian welfare state and history of Vikings is not the first place you associate with libertarians. However the International Alliance of Libertarian Parties does have a representative from the land of the fjords. The Capitalist Party (Liberalistene) (Wikipedia), advocates for a minimal state and free market economics. We speak with Deputy Chair Political, Roald Ribe about the party.
Roald thank-you for your time.
Could you tell our readers about your party?
A huge mix of value-liberal, classical liberal, libertarian, minarchist, anarchist, laissez-faire, individualism oriented capitalists. Common ground is typically no rulers, less government, less laws and regulations, less tax, less bureaucracy, less politicians and so on. Unyielding on principles, on property rights and self-ownership, but flexible on speed of implementation. It will take time to provide enough people with enough knowledge to let them realize that they want anything to change, or to recognize the fact that a better society could and can exist. Our political programs are evolving significantly over time (7 years so far) to reflect that fact, and to try to factor some acceptance of the Overton Window into them and the general communication with potential members and voters. Our name in Norway is Liberalistene. In English the name is Capitalist Party. Where Laissez-faire is implicit in the name.
“Getting representation for a classical liberal ideological base into the public view, always insisting on less state, less taxes, less power to politicians and bureaucrats, gets our membership (and me) excited”
What are main issues in Norway you campaign on, what gets Libertarians excided?
We have distinct political programs covering most issues on three political levels (all) in Norway. Three levels seems a bit much for just over 5 million people, so we will try to merge the two lower into a local level, and the other a national level like today. As a start. All the “established” parties in Norway, those who are represented in parliament most of the time, seem to agree that there is no maximum size for the state in the economy. Creating a heard voice, a rallying point, recognised representatives of the opposite view, is task number one. Getting representation for a classical liberal ideological base into the public view, always insisting on less state, less taxes, less power to politicians and bureaucrats, gets our membership (and me) excited.
Your country has stayed out of the EU, but what’s your parties view of the EU and the Euro?
The population in Norway has voted against joining the EU twice. Political representatives in parliament still slipped Norway in, through the small back door named the EFTA, with no asking the population again first. Probably because they expected that the answer would be the same as for the EU. So, we are part of the EU, but “only” through the EFTA. There is a majority for it in Norway it seems (EFTA), because voters have bought the political dogma that Norway “needs” such a deal to sell oil, gas, fish, electrical power and other unrefined and raw materials into the EU area or other parts of the world. It will not take much free market knowledge to realize that this is an outright lie. So, we are in the EU, but with no influence. Our party would strongly prefer for Norway to be out of that situation.
Different countries campaign in elections in different ways, what methods does your party focus on, and do you have any interesting stories from the campaign trail?
Our next national election for parliament is in this year, 2021. So we are in the middle of preparing for it now. The formal election campaign lasts from 10. August till the election day 13. September. Most significant boost in this election campaign is that a former Minister and MP with 20 years of experience in parliament, has joined our party. Mr Per Sandberg used to be Deputy Chair of the Progress Party, but has now upgraded himself ? to the top election candidate for Liberalistene in the Oslo and Finnmark election districts. This has not gone unnoticed in the media, and through his activities combined with our steadily increasing experience with media handling and election processes and campaigns, we get a lot more attention and traction in the media than we have been used to this far.
In addition to the constant hard work leading up to being taken seriously enough to be joined by an established political figure, campaigning is done in various physical forms. Branded stands in streets where we have enough active people to swing it. Talking to people, distributing brochures. In some less urban areas we are getting a lot of brochures distributed straight into mailboxes by single activists. We try to write opinion pieces for different news media, and we are getting better at it. With a couple of pre-qualified celebrities in our ranks, it is getting somewhat easier to get the party included in the media.
At this point in time we do not have the capacity to make a trail of it. In the locations where we have enough active personnel, they organise their own plans and activities in their area, basing the plan on their own assessment of when, how and what kind of effort can be realized by them, and what they think will be most effective there. The central / national organization is mostly a service and materials provider, making brochures and flyers available, ordering tents, flags and other materials in ways that makes it affordable and available for as many as possible.
“It will be interesting to see what kind of trade relations the UK develops with the world going forward by itself outside of the EU. If the UK is successful with that work, as I expect it to be, it may undermine the solid political EFTA support in Norway, which would be perceived as a good thing by our party”
Do you have any views on UK politics you can share?
I think your country did well to finally get the Brexit process into motion, but I expect that the usual suspects will drag their feet and silently sabotage it as much as possible. It is nice to observe that some of your political figures seem to wise up a bit on lockdown policies. It is about (bleeping) time… It will be interesting to see what kind of trade relations the UK develops with the world going forward by itself outside of the EU. If the UK is successful with that work, as I expect it to be, it may undermine the solid political EFTA support in Norway, which would be perceived as a good thing by our party. We hope our countries will continue to uphold the traditionally good relations between them, and continue to work for the best possible conditions for cooperation between the two populations, including as much free trade as possible.
If you could introduce, repeal or change 3 laws what would they be?
A law securing absolute property rights, protecting all possible value from coerced confiscation, especially from the government.
A new law securing negative rights only for individuals exclusively, abolishing any and all privileges given in law to any individual or group.
A new law to require that at least two old laws must be removed for new or changed to be introduced.
“Governments have lost their last marbles if it ever had any, and are flushing down the economic future of many in a hole full of dirty, irrational, fear mongering. The only way to counter this is to provide more individual freedom and economic freedom for business”
Lastly how do you think your government is handling the Covid-19 crisis, and what would you like to done to help the economic recovery?
Lockdown is a travesty against citizens, especially those in the low income bracket. The only rational strategy out there seems to be The Great Barrington Declaration. Governments have lost their last marbles if it ever had any, and are flushing down the economic future of many in a hole full of dirty, irrational, fear mongering. The only way to counter this is to provide more individual freedom and economic freedom for business. Failure to do so should eventually be punished by quite a few voters. In that path, where we expect more voters to arrive eventually, is where libertarian efforts should loudly position themselves. But remember, voters go where they believe is right, not where you think they should. We must make it our business to find the points where those two often differing views coincide with each other, well in advance of voters arriving there.
The TaxPayers’ Alliance has called for tax cuts to support Britain’s pubs. They have also issued new beer mats, which will be distributed in pubs across the country urging punters to sign their petition. Speaking to the invited audience at the Barley Mow pub, chairman and founder of JD Wetherspoon Tim Martin was adamant that if Britain’s boozers are to survive, the government must help this struggling sector.
Dan was there to report:
“It was fantastic to be able to join the TPA for the launch of their “Quids Inn” campaign. After the last 16 months of lockdowns everybody certainly deserved a drink! The current VAT reduction really should be extended beyond September to enable the hospitality industry to recover from the pandemic.
It was also great to catch up with so many stalwarts of the cause of freedom. It is clear we are going to have to work together to ensure a classically liberal approach to the nation’s post-Covid future.”
On the 21st June, 2021, Labour MP Emily Thornberry appeared on BBC radio 4, insisting that the government must cease the lifting of protections in place for British Steel; stating that:
“We have to stop this government lifting the protections that steel has at the moment, because if we don’t, then we could end up with cheap steel being dumped in this country and it being the end of the steel industry.”
Throughout the Free Trade talks with Australia as well, farmers unions have been demanding for greater protections to be in place, with suggestions of restrictions on the number of meat produce that can be imported into the country, while allowing the free export of British meat.
One has to ask whether we’re seeing a return to Protectionism and Mercantilism.
In a sense the UK has never truly abandoned fallacious positions of trade. The British Steel industry has a history of bail outs and subsidies; in 2019 the government issued British Steel a £300 million bailout. In the same year, it received £43 million in subsidies.
But what is Protectionism, and what is Mercantilism?
Protectionism is idea that government must implement policies that restrict international trade, with the guise of helping domestic industries, and protecting consumers from making “harmful” choices.
Mercantilism is an economic policy designed to maximise the exports of the nation and minimise the imports to said nation, via regulations, tariffs, and to a degree outright bans of imports for certain goods.
On the surface there is very little difference between the two positions, as in the end both stifle competition and offer privileges to protected industries.
The conclusion from many Protectionists and Mercantilists is to issue tariffs on foreign imports, and offer subsidies to national industries in order to avoid a trade deficit, and have fair competition.
“domestic consumers face the costs of these tariffs, as they find the goods and services they wish to buy cost more; thereby reducing the consumers standard of living”
Tariffs however, hurt a nations consumers. While the country’s government in question may issue tariffs for the purposes of protecting domestic industries and consumers from apparent “dumping”, the domestic consumers face the costs of these tariffs, as they find the goods and services they wish to buy cost more; thereby reducing the consumers standard of living.
The issue of subsidies has a similar effect on consumers. A subsidy at the end of the day is a tax, and by extorting from consumers in order to prop-up a domestic industry, you’re reducing their expendable income.
The area Protectionists wish to avoid however, that of a trade deficit, is fallacious at best. The trade deficit myth looks at purely the flow of financial capital from one nation to another, yet it fails to look at why money is flowing and what those who transferred capital received in return; that being, the goods; whether that be goods of higher order for the purposes of more efficient production processes, or lower order goods (final goods: consumer goods). The problem with the concept of a trade deficit is, it answers too much: If more money via trade flowing from one country to another, while disregarding the goods received is a serious issue, then we must also look at the trade deficit between England and Scotland; or London and Oxford.
“the trade deficit doctrines logic, I have a trade deficit with the hobby business, Games Workshop. Over the course of 10 years, I’ve probably given £50,000 to the company. We have to ignore the products I received in exchange”
By the trade deficit doctrines logic, I have a trade deficit with the hobby business, Games Workshop. Over the course of 10 years, I’ve probably given £50,000 to the company. We have to ignore the products I received in exchange, and all the subjective value I attained from these goods, and time spent utilising them; we should only look at the movement of money. I need to issue quotas against Games Workshop of how many goods they’re allowed to sell me, in order for the payments between me and them to equalise.
The ends which Protectionists wish to reach, is that which they loosely label “fair competition”. The problem is, their concept of fair competition is not only far from any meaning of fair; as it requires the protection of some industries and barriers in place of others, but, also that the fair competition doctrine is very similar to the idea of perfect competition.
The theory of Perfect Competition is the state of affairs, where there are a certain number of buyers and sellers, selling (buying) the same quantities for the same price. The question that arises is; where is the competition?
The market is not a state of affairs; it is a process of discovery. To get right to the core of the problem with this doctrine, via the perfect competition doctrine, you rule out the possibility of the entrepreneur discovering an absence of information that is held by consumers and his competitors. Under the perfect (“fair”) competition doctrine, it is attempted to maintain what could be called a static form of the market; the subjective values, marginal utilities and choices of consumers, and the multi-period production processes of competitors put a wedge in your plans. Consumers have made the “wrong” choices; competitive entrepreneurial producers have discovered how to sell the same product cheaper – it’s not “fair”.
The Market is a process of discovery. At any moment, market participants can face utter ignorance; not just that of optimal ignorance – where participants know what they don’t know, but the costs outweigh the gains, but that of an absence of information; we do not know what we don’t know.
It is the role of the entrepreneur to be alert to the ignorance of market participants, and predict what the future price and value of goods will be. It is the role of the entrepreneur to see incoordination in the market – where there are two prices for the same good; indicating to the entrepreneur that sellers(buyers) are offering(charging) too high(low) a price; if he is alert and sees one selling for 20 and one for 10, he will buy at 10 and sell for 15. It is through this entrepreneurial process of discovery, that we move away from disequilibrium and closer to equilibrium.
There is not just the pure entrepreneur who sees sellers, one at 10 and one at 20 and chooses to sell at 15. The entrepreneurial producer discovers he can produce the same product for a lower price, and the entrepreneurial seller may request his employees to smile more to appear friendlier in order to sell more goods.
The only way to allow the market process to operate, and to have entrepreneurial discovery is to have actual “fair” competition, which is freedom of entry; i.e. no privileges.
That which is often; intentionally or not, overlooked, ignored, and disregarded by the Protectionists; Consumer Sovereignty, must be stressed here.
“Consumer sovereignty is often something that Interventionists of all stripes; no matter the term we use, wish to stamp out. …Consumers vote with their feet and wallets”
Consumer sovereignty is often something that Interventionists of all stripes; no matter the term we use, wish to stamp out. Consumers ultimately have the final say of which goods are produced; how successful a production processes product will be, and who provides greater value via the epistemic nature and signal of profits. Consumers vote with their feet and wallets.
There is an entrepreneurial aspect to the consumers as well as those mentioned previously. An entrepreneurial consumer, who discovers he can satisfy his wants/needs for a cheaper price, will seek to obtain these means to satisfy his wants, and utilise them for the value they achieve, and profits from their service to him.
The practices of the Protectionist and the Mercantilist require denying the consumer of his sovereignty, and to classify the praxeological aspect of the consumers’ choice as wrong; the interventionist ideals of these two require not only the denial of consumer sovereignty, but the denial of subjective value.
– Is Our Core Argument Based On Efficiency? –
The answer to this question, to which we’ll finish with, is in the negative. The core of the argument for free trade is the same as that for the market process as a whole: coordination.
The purpose behind why the free market in all areas is the superior system; including that of trade, is because it better achieves coordination of the subjective values of individuals. The free market, through the entrepreneurial process of discovery, and the freedom of entry into the competitive market, allows for greater ability to coordinate market signals, and Protectionism stifles with this coordination; placing static over the signals and providing false or faulty signals – in total reducing the quality and leaving values unsatisfied.
It is for coordination that we should reject Interventionism in all its forms; whether it be Protectionism, Mercantilism, or Nationalism.
– This Piece Is Satire and Should Not Be Taken Seriously –
– If You Do Take This Piece Seriously, Please Thoroughly Research The Term ‘Satire’ –
– Dedicated To Jessi Bennett. You Made Me Do This –
Human life, as all life, faces a time constraint; it is in large part due to this constraint that humans rely on their subjective time preference with regards to the choice for current consumption or future consumption.
To add to this, the time preference over current/future consumption is what makes interest rates possible. The time preference aspect of interest is based on the notion that humans’ prefer to consume in the present, rather than at a designated later, future time period; it is this time preference which helps to explain monthly payments of, for example, a TV.
(Due to time preference, people tend to accept small payments over a set time period for full ownership in the future, i.e. £500 for a TV to buy it in the present, or a £50 deposit followed by monthly payments plus interest, unless ceteris paribus, their ordinal ranking of the good is high, as well as the demand to satisfy their wants/needs for current consumption, i.e. they’re not willing to postpone; people would not be willing to pay the final settlement price for a good they want to satisfy their wants now, if they have to wait for the future to receive the good)
What would happen though, if some genius entrepreneur discovered a way to make humans immortal?
“Governments would hate it because they wouldn’t be able to issue a Death Tax or Inheritance Tax, so they would probably try to ban it”
Firstly Governments would hate it because they wouldn’t be able to issue a Death Tax or Inheritance Tax, so they would probably try to ban it, it would then enter the black market and cartels would tamper with it and turn everyone into zombies.
But assuming Governments don’t interfere (I know, it’s a big assumption more unlikely and unrealistic than this piece), the other question to ask is, how immortal would it make people? Would it be a simple case of humans wouldn’t die of old age, but could die from starvation and disease, or, would it be a case of complete immortality; no disease, mortal wound, aging, or level of hunger could kill a human?
We’ll assume it to be the more simple case, since it’s easier to grasp and if we assumed complete immortality, then the Hyperventilating Overpopulation Ensemble (HOE) would have a heart attack.
“we would likely see a large shift in the market from current consumption to future consumption, with the time preference for goods and services extending for future periods of ownership and consumption”
If humans had the basic degree of immortality (cannot die of old-age, but can from mortal wounds, starvation and disease), then since the time constraint of life would be unaffected by old age, while the time preference and marginal utility of food and medicine would remain the same, we would likely see a large shift in the market from current consumption to future consumption, with the time preference for goods and services extending for future periods of ownership and consumption.
Under this assumption, since peoples’ time preference as a whole has seen a shift to the future, if people still prefer small payments over a prolonged time period, then we would likely see, ceteris paribusinterest rates plummet, since people would be saving far more than they are spending; meaning an exponentially larger pool of funds, would be available for long-run multi-period projects of production, expansions in capital goods for larger scale productions of consumer goods in the future, a larger housing supply etc.
In conclusion: I the writer clearly need to get out more.
We are joined by Steve Kelleher, the recent London Mayoral candidate for the SDP, and Scott Neville, the Co-Founder of the Hampshire Independents, as we discuss the lack of an effective opposition to the current Government and where a future opposition might come from.
Fact: Most politicians know very little about Medical Science and Technology.
Fact: Politicians consult committees of experts to advise them on any complex subject.
Fact: Most of the members of a committee set up to advise on Medical Science are representatives of pharmaceutical companies.
Question: Are they going to advance the agenda of people like you and me or their agenda and that of their shareholders?
Pharma reps have tried it on a few times before with SARS, Bird ‘flu and Swine ‘flu. They did a pretty good job of terrifying the Blair/Bown government with Swine ‘flu and managed to con them into buying £1.2 Billion pounds worth of pointless vaccine but it didn’t take long before the jig was up. The public began to see through it and an embarrassed government quietly swept it under the carpet.
But, learning from their mistakes, the Pharma reps have done a much better job with Corona Virus/Covid 19.
1. They avoided the word ”flu’ – far too familiar
2. They recommended complete lockdown – a masterstroke, making people desperate to get on with their businesses, their lives and, of course, their holidays!
3. And then there’s the statistics!
To get the statistics into proportion, let’s compare Covid-19 to pneumonia.
Most people on their deathbeds are either in the 70+ age group or have compromised health conditions. These people are usually pushed over the edge by pneumonia or influenza and that is written on the death certificate as cause of death.
Do we then conclude that there is a pneumonia pandemic? No. Instead of going into a blind panic, we see the figures for what they are.
With impressive sleight of hand, the rather similar Covid figures have been INTERPRETED DIFFERENTLY. In cases where Covid-19 has precipitated the deaths of dying people, it has been interpreted that there is a PANDEMIC.
But it gets worse. Having been instructed by our terrified politicians that the global pandemic is ‘a fact’, the usually dependable Office of National Statistics gets caught up in the panic too.
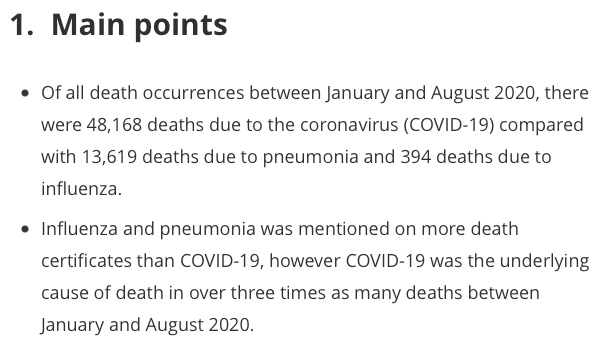
I consulted them for some figures and screenshot twp paragraphs.
When I saw the first paragraph, I thought that maybe I’d got it wrong but THEN I read the truly shocking second paragraph. It tells us that:
In most cases, these highly trained and experienced doctors diagnosed that the patients died of PNEUMONIA OR INFLUENZA and NOT Covid 19! But then…
A civil servant at the ONS, who I am willing to bet good money was NOT present at any of those deaths, tells us that these doctors GOT IT WRONG!
He tells us that although influenza or pneumonia was entered on the death certificate as the cause of death, “COVID-19 was the UNDERLYINGcause of death…”
How could he possibly know this? He didn’t. This is a perfect TRIUMPH OF BELIEF OVER FACT.
Having ‘statistically proven’ that there is a pandemic, pharma companies have done their best to discredit the cheap, safe, tried and tested treatments which are outside of their licences, promoted new, expensive vaccines and laughed all the way to the bank.
The global economy has been shaken, innumerable people have lost their livelihoods and the pharmaceutical companies’ shareholders have never been happier.
And now vaccine passports? This will be a bonanza for tech companies but is a seriously dangerous precedent. It will be a loss of civil liberty which will increase over time. People will be forced into being vaccinated under threat of not being able to fly, work or socialise. It will be a GOVERNMENT SANCTION OF ASSAULT.
If people want to be vaccinated, let them.
But if they want not to be vaccinated, let them not.
Your hero, Winston Churchill ENDEDID. Cards after WW2. Please do not go down in history as the prime minister who not only brought them back but forced people to receive an incompletely tested vaccine against their will.
There must be no vaccine passports and no employer, airline or any other institution should be allowed to use non vaccination as a justification to refuse access.
Now we hear “Significant sums” are still being queried by auditors in Croydon LBC’s 2019-20 accounts – with the auditor having sought advice from a QC over one outstanding issue – while a number of “significant risks” remain over the current year’s budget”
The Chronicle reports: “concerns around the approval of a £30m refurbishment budget for the council’s Fairfield Halls arts centre, to be paid for through the transfer of land to Brick by Brick to be developed and sold” and that “there are “a number of significant risks, amounting to £26.6m, which could negatively impact on the outturn position” – even before any accounting adjustments needed for the Fairfield Halls development are taken into account” compared to reserves of just £7.4 million.
It has now been almost 10 months since we first spoke of the imminent de facto bankruptcy of the council. We now have to ask, what has changed in that time? How have the finances of local taxpayers’, and the needs of service users been protected? Why has it taken 10 months for these issues to come to light? We want to know why weren’t the fully extent of the problems made clear when the councils finances were first recapitalised, and how can we fell confident we will ever see an end to this ongoing failure of governance?
We have now regained our nations independence and fully left. In commemoration of the 5 years since the vote, we’re proposing to go for drinks in what during the campaign became Croydon’s Brexit central, the Skylark.
We don’t yet know what lockdown restrictions we will be operating under. As such we’re not able to book an area, however we propose to be at the Skylark (34–36 South End, Croydon, CR0 1DP) on Wednesday June 23rd from 7pm, and will operate under whatever rules we need to. Feel free to come and join us.
Mike & Dan meet up in the Foxley Hatch in Purley, to discuss the achievements of the Croydon Constitutionalists in our third year and our hopes for the year ahead.
No subject could be more controversial to discuss in the UK more than reforming; or abolishing the NHS. The NHS has existed for over 70 years, and over that time the British people have insisted in telling themselves that, they have ‘the best healthcare system’, and that the NHS is ‘the envy of the world’.
The only problem is…none of this is even close to being true.
“The idea that the organised working classes were demanding a government takeover of healthcare is a post-hoc rationalisation, which projects the fondness for the NHS, which the public subsequently developed, back into the period of its creation”
We continue to tell ourselves that the NHS was the great achievement of the working classes; rising up and demanding national healthcare, in which free access would give power to the people. But, as Kristian Niemietz of the Institute of Economic Affairs points out:
“The creation of the NHS had little to do with pressure from below; it was not a change that ordinary people had fought for. Far from being People Power in action, the NHS was a brainchild of social elites, to which the general public just passively acquiesced. The idea that the organised working classes were demanding a government takeover of healthcare is a post-hoc rationalisation, which projects the fondness for the NHS, which the public subsequently developed, back into the period of its creation.” (Kristian Niemietz. Universal Healthcare Without the NHS. p. 19)
Nick Hayes has reiterated this ex-post rationalisation; explaining that huge support for a nationalised health system was merely a pipe dream piece of propaganda:
“The evidence before us seems to indicate a fairly large amount of resistance to State interference in the field of medicine […] roughly half the population was opposed to any major change on the health front, a quarter disinterested and a quarter in favour of State intervention.” (Nick Hayes. English Historical Review. p. 659)
Evidence in our modern times, gives an interesting expansion on this. The British Social Attitudes Survey (2015) reveals when members of the public, are asked if they would hold a preference for being treated by an NHS-based provider of healthcare, a private profit driven, or a private non-profit provider, 43% state no general preference. A further 18% provide an explicit preference for independent, non-state-based providers of healthcare.
The phony info from NHS propagandists’ continues. The system prior to the creation of the NHS was not a bleak world where people died in the streets; desperately searching for a doctor only to find none exist. Before 1948, the health system operating in the UK was well developed. The system was rooted in the mutualism of the 19th century. The creation of the NHS was not the development of a new system; it was simply a government takeover.
Let’s get back to the common phrase mentioned earlier: the NHS is the envy of the world. The argument is that the NHS is the envy of the world, due to instituting a system, which does not base its service on an individual’s ability to pay for said service. This is treated as an outstanding achievement, yet the vast majority of the developed world has universal access to healthcare (the US is the exception, but we will come to that later). Are we not begging the question of how the NHS is the envy of the world, when the reality of the developed world’s health systems indicates otherwise? Your neighbour can hardly envy you for what you have, if he already has it.
“if the NHS is the envy of the world, then why is it, after over 70 years no developed nation has copied the structure the UK has; why does it refuse to copy the system it apparently envies so much?”
Furthermore, if the NHS is the envy of the world, then why is it, after over 70 years no developed nation has copied the structure the UK has; why does it refuse to copy the system it apparently envies so much? The answer comes in two:
(1) Other developed nations understand there is a difference between universal access as a standard, and the nationalisation of healthcare.
(2) The NHS is not the envy of the world; nor has it ever been.
The NHS is not just far from the envy of the world when looking at the universal healthcare status of other developed nations, but according to the OECD, the UK has one of the worst healthcare systems within the developed world. When the report was first published, The Independent stated:
“The quality of care in the UK is “poor to mediocre” across several key health areas […] and the NHS struggles to get even the “basics” right […] Britain was placed on a par with Chile and Poland.”
The Financial Times in addition reported on the findings; stating the following:
“Britons are less likely to survive a heart attack, stroke and leading cancers than people in many other developed nations, according to an assessment of international health systems”
Many apologists for the NHS, would be quick to point to the Commonwealth Fund Study; proclaiming that the CFS “proved” that the NHS is the best system in the world, because it was ranked 1st.
This completely ignores that the CFS looked at inputs, not outcomes. When it came to the one category which looked at outcomes, the UK came out second to last, only slightly above the US. In addition the Commonwealth Fund Study was designed to systematically favour healthcare systems which are tax-funded. The CFS asked patients if their insurer ever declined payment for treatment, and whether they have ever incurred out of pocket payments in excess of over £1,000. These declining of payments and out of pocket payments, would not only be almost impossible under the NHS, but under the systems of Sweden and Norway also. Looking to the CFS for neutrality is like looking to the Central Bank of England for financial stability; you have to lie and make assumptions that fit the outcome you want. The CFS held a category for cost issues titled ‘Cost-Related Access Problems’; this however is based on price limitations with regards to consumers, and mentions nothing on the matter of non-cost based restrictions, such as state rationing.
Many proponents of the current system, when presented with this information, would be quick to state: “okay sure, the NHS has some problems, but that’s just because of underfunding and the spending being cut.”
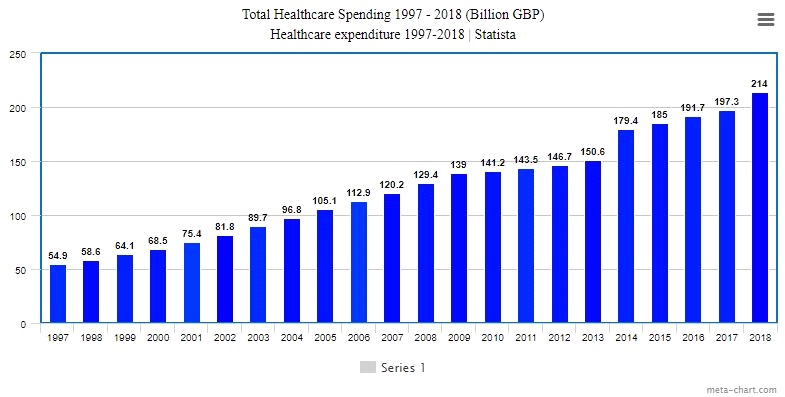
“In 2018, spending on the NHS was £214 billion; an increase in spending of 296% over a 20 year period. If there has been a cut in spending on the NHS, I’m failing to see where it is”
Well, reality paints a different picture.
According to data from Statista, from the period of 1997 to 2018, spending on the NHS has been on a continuous increase, as shown below:
As shown in the data, in 1997, spending on the NHS was at roughly £54.9 billion, and has been on a consistent rise. In 2018, spending on the NHS was £214 billion; an increase in spending of 296% over a 20 year period. If there has been a cut in spending on the NHS, I’m failing to see where it is.
Before we touch on the US healthcare system, and the myth of it being a free market system, I think the reader would agree it is important to “put my money where my mouth is”, and provide examples of how the NHS fares compared to other developed nations.
The next few sections will look at the following:
NHS Outcomes Compared to Other Developed Nations.
The Universal Systems of Other Developed Nations
After we’ve discussed the US healthcare system, we will go over potential reforms and alternative means of providing healthcare, while keeping the essence of universality.
NHS Outcomes Compared to Other Developed Nations
Let’s take a look at performance rates of the NHS and other systems.
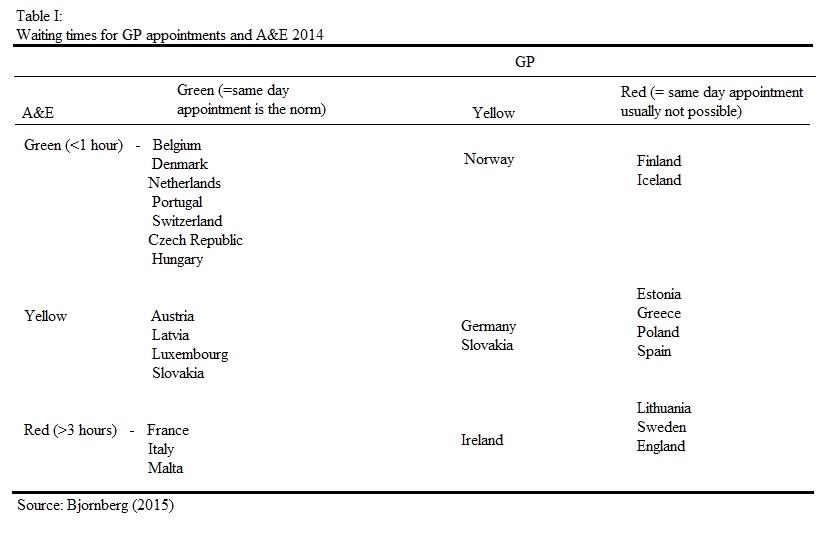
The above table showcases how countries’ healthcare systems compare when it comes to waiting times for GP appointments and A&E.
Nations marked as green indicate an average waiting time of less than 1 hour, yellow in between 1 – 3 hours, and red over 3 hours.
As we can see, the top performers are Belgium, Denmark, Portugal, Switzerland, the Czech Republic, and Hungary. The worst performers include Lithuania, Sweden, and England. Under the NHS, obtaining a same day appointment to see a GP is close to impossible, and waiting times in A&E on average are over 3 hours.
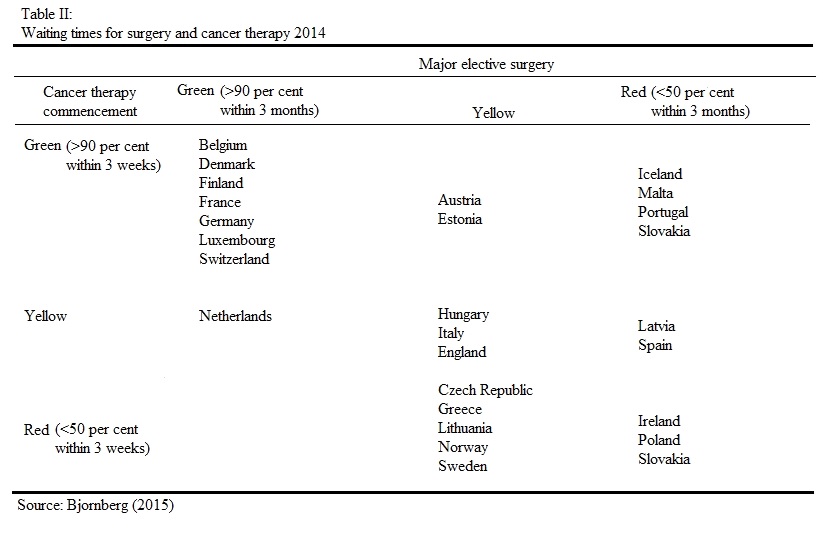
In the second table we look at the waiting times for surgeries and cancer therapies. The top performers here are: Belgium, Denmark, Finland, France, Germany and others. The worst performers include Ireland, Poland, and Slovakia. The NHS rates yellow, meaning roughly 50% can be conducted within 3 months.
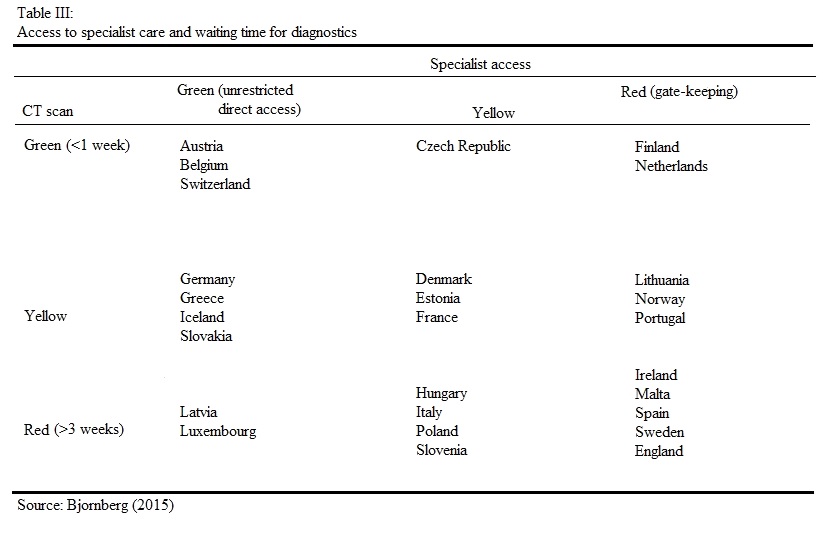
The third table looks at the waiting time for diagnostics, and how easy it is to receive specialist care; if a patient can access such care directly, or if there is gate-keeping in place such as going through a GP.
The top systems in this regard are Austria, Belgium and Switzerland. The longest waiting times for diagnostics and restrictions in place for accessing specialist care occur in Ireland, Malta, Spain, Sweden and England.
Throughout all of these areas, many systems dip between green and yellow, some more than others consistently keeping in the green. The NHS on the other hand, the majority of the time remains in the red, with only one example of being in the middle (yellow).
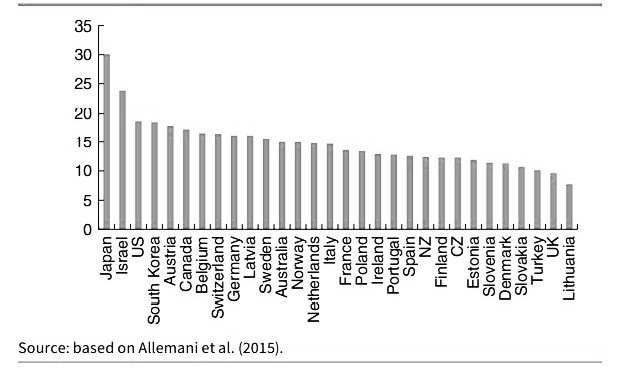
We’ve taken a look at waiting times, what about survival rates? Let’s take a look at cancers first.
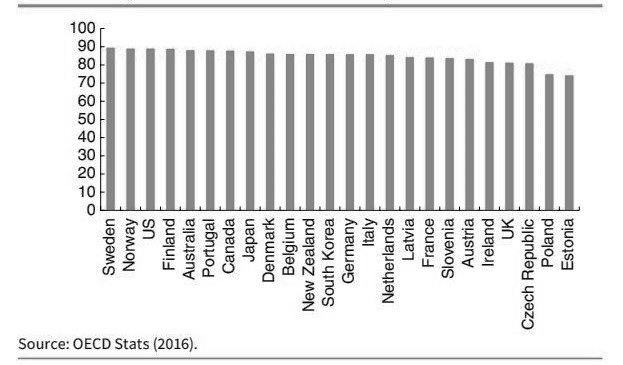
In the UK the most common form of cancer is breast cancer. The diagram above shows the 5 year survival rate for breast cancer patients. The UK’s survival rate is 81.1%; roughly 5% behind South Korea, and roughly 2% behind Austria; if NHS patients had been treated under the South Korean system, we can speculate roughly 2,500 lives could have been saved, and extended every year.
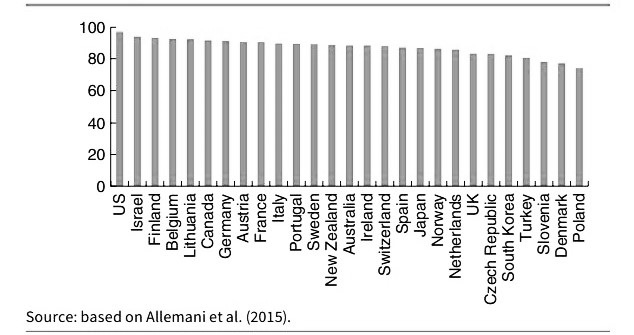
The second diagram shows the five year survival rate for prostate cancer. Under the NHS system, the survival rate is 83%, which is lower than most of the developed world. For patients in Sweden which ranks 12th in the diagram, the survival rate is roughly 6% higher. We can estimate that if NHS patients were treated there, a further 2,800 could have survived.
Lung cancer is next on the list. The UK has a survival rate of less than 10%, making it the worst performing compared to all high income, developed nations. Roughly 2,400 additional lives could have been saved under the Australian system, which is 5% higher than the UK.
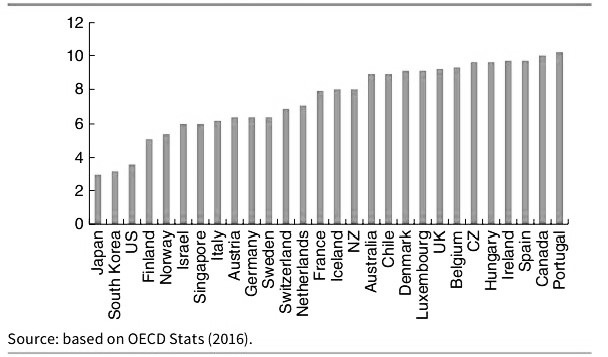
Let us take a look at stroke mortality rates:
Ischaemic strokes are one of the most common types of stroke in the UK, with roughly 150,000 cases per year (Stroke Association 2016). The UK has a survival rate of 9%. Again, if NHS patients were treated in Sweden, around 3,000 extra lives could have survived an Ischaemic stroke.
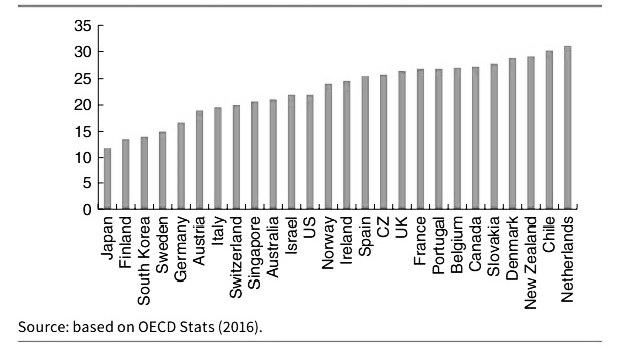
Finally, we look at the mortality rate for Haemorrhagic strokes. The UK, once again, is a poor performer for survival. The UK has a mortality rate of 26.5%, which is over 4% higher than the US; translating to roughly 1,000 excess deaths.
“The systems of Switzerland, the Netherlands, Germany and Belgium, can be described under a broad term of operating under Social Health Insurance systems. In the rankings previously shown, these countries have consistently outperformed the NHS”
The Universal Systems of Other Developed Nations
We’ve looked at survival rates and mortality under the NHS system, and so we shall now go over what the universal character of other developed nations looks like.
The systems of Switzerland, the Netherlands, Germany and Belgium, can be described under a broad term of operating under Social Health Insurance systems. In the rankings previously shown, these countries have consistently outperformed the NHS.
How Does Social Health Insurance Work?
Social Health Insurance works a similar way to standard insurance. There are however a few unique qualities which are:
Community Rating: Under a SHI system, insurance companies cannot raise premiums based on an individual’s health risks.
Obligation to Accept: SHI systems prohibit insurers from rejecting coverage based on an individual’s medical history.
No Exclusion: Pre-existing conditions cannot be denied for coverage under a system of SHI.
Individual Mandate: Under a SHI system, it is compulsory for all individuals to purchase SHI, and is mandated by the state. If an individual does not purchase SHI, then they are put on one automatically; even against their will.
Premium Subsidies: Due to the point of mandates, the government subsidises the SHI of people on low incomes. For some nations this is a means-tested based subsidy, in others it is income dependent.
Under the Swiss system of SHI, it could be argued there is a higher degree of freedom of choice for patients than in other SHI systems, including a cost-sharing measure worth looking into. Out-of-pocket payments under the Swiss SHI, account for roughly a quarter of total healthcare spending (according to W.H.O 2015: 132-133). This system has two distinct components: deductible and proportional co-payments. Deductible works similar to most insurance systems with excess; there is a minimum cost threshold which, once costs exceed this, the insurance covers the excess costs. People can freely have a higher minimum threshold set, in return for premium rebates.
Co-Payments are capped at a certain amount per year. Once a patient’s collective medical bills reach said amount, then they face no further expenses.
“In order to prevent the cost of healthcare rising exponentially during old age, German PKV insurers are required to smooth premiums over people’s lifetime. This “pre-funding” mechanism works in a similar way to a pension”
The German health system has two types of healthcare coverage. These are the standard type of Social Health Insurance; known as GKV, with the community rated premiums and other qualities mentioned above, and a conventional, private health insurance; known as PKV, with varying premiums, and no risk compensation.
Additionally, the German system has a quality that many nations could learn from: an accumulation of old-age reserves. We understand that healthcare costs are flat for the majority of life (not including exceptions), and then rise with age. In order to prevent the cost of healthcare rising exponentially during old age, German PKV insurers are required to smooth premiums over people’s lifetime. This “pre-funding” mechanism works in a similar way to a pension; insurance companies build up an old-age fund on behalf of their clients during their working life, and later draw on this fund for care during old age.
Before we go into the US, I want to briefly talk about the South Korean system.
South Korea has a universal health insurance system, similar to that of SHI; the difference being though, is that the state is unable to set market prices. Many Koreans seek additional private coverage due to the state-based insurance being insufficient to cover all the costs; around 8 out of 10 Koreans take out private coverage, with an average cost of 120,000 Won (£75) a month.
Care in South Korea is provided by hospitals which are 94% private, a fee-for-service model and no direct subsidies. This private system is not purely for-profit, the Korean system has a mix between for-profit, non-profit and charity foundations. The presence of private hospitals expanded in the early 2000s; from 2002 to 2012, private hospitals rose from 1,185 to 3,048. Further information on the South Korean system with a comparison to Italy, and a look at how it handled the outbreak of Covid-19, can be found here:
Most of the time NHS propagandists will point to the US and decree: “See! That’s free market healthcare for you! If we didn’t have the NHS (praise be upon it) then we’d have a US system!”
There are two problems. firstly, NHS propagandists intentionally ignore the vast majority of other SHI systems which outperform the UK; relying on the publics ignorance of other systems outside the UK and US. Secondly, the US has not had anything close to a free market in healthcare for at least 100 years. It has become an interventionist, heavily regulated system with positions on competition similar to that (which I’ve discussed a fair number of times) of Neo-Classical General Equilibrium Theory and Perfect Competition. I won’t go into the subject in order to save the reader time, but if you’re interested in understanding what I’m referring to, you can check out my article where I discuss it in detail here – https://croydonconstitutionalists.uk/marshallian-curve/
As was mentioned above, the United States has not held a free market in healthcare since 100 years ago. Jacob Hornberger, the founder and president of the Future of Freedom Foundation, gives a mention to this in his book, The Dangers of Socialized Medicine:
“For over one hundred years, the American people said no to governmental intervention into health care. Americans did not permit their respective states to licence physicians and other health-care providers. They did not permit government to provide health care to the poor and needy. No one was required to purchase health insurance.” (Jacob Hornberger. The Dangers of Socialized Medicine. p. 15)
The government has always attempted to interfere in healthcare, including various lobby groups and unions wishing to curtail care with the use of government power, however it could be argued the defining moment American healthcare changed for the worst forever was the successful lobbying done by the American Medical Association. To further quote Mr Hornberger, he goes into great detail on the impact the AMA had on healthcare in the US:
“The American Medical Association is perhaps the strongest trade union in the United States. The essence of the power of a trade union is its power to restrict the number who may engage in a particular occupation. This restriction may be exercised indirectly by being able to enforce a wage rate higher than would otherwise prevail. If such a wage rate can be enforced, it will reduce the number of people who can get jobs and thus indirectly the number of people pursuing the occupation. This technique of restriction has disadvantages. There is always a dissatisfied fringe of people who are trying to get into the occupation. A trade union is much better off if it can limit directly the number of people who enter the occupation-who ever try to get jobs in it. The disgruntled and dissatisfied are excluded at the outset, and the union does not have to worry about them” (Jacob Hornberger. The Dangers of Socialized Medicine. p. 65)
“the number of medical schools in the US, from the period of 1910 to 1920 dropped from 131 to 85. This cut in medical schools not only had; and continues to have, a supply-side effect by causing prices to artificially be forced up”
The AMA’s successful lobbying campaign, was to restrict the number of doctors who could enter the medical profession by drastically reducing the number of medical schools in the country, and enforcing mandatory licencing into the nation. After the successful lobbying for accreditation was granted, the number of medical schools in the US, from the period of 1910 to 1920 dropped from 131 to 85. This cut in medical schools not only had; and continues to have, a supply-side effect by causing prices to artificially be forced up, it had a huge impact on women and African Americans entering the medical profession. By the time of 1944, the total number of medical schools which admitted black people was cut from 7 to 2.
Many may argue that licencing is good particularly for healthcare. But a licence does nothing to prove a doctor is competent. A doctor could have been in the medical profession for 30 years and be completely incompetent. Two types of objections can be made against licencing:
Economic Objections | Licencing puts a gap between patients and healthcare providers. By restricting the trade of healthcare through additional costs for licencing, it reduces the supply; by reducing the supply this, as stated previously, artificially forces the price up. This added cost is passed on to the consumers of healthcare services. This barrier to entry goes completely against the freedom of entry required for a competitive market to function, under entrepreneurial discovery.
Social Objections | Licencing gives a false sense of security to patients that lead to unfulfilled expectations of doctors being medical automatons; incapable of making human errors and bringing nothing but unnatural perfection to the table. This can harm the relationship between the doctor and patient; causing high dependency and resentment. Furthermore licencing as indicated above, discriminates against not only African Americans and women, but poor people too. While it has been used to keep women and minorities out of the medical profession in the past, the continued effect it has on the poor, is to force them out of the market through disincentives; via expensive education and other requirements for licencing.
Licencing, to some up, is designed to keep doctors free from competition, and increase their wages, through the means of the government giving out privileges and putting up barriers to entry. It is a throwback to the old, European Guild system, and has made the healthcare market aristocratic.
To quote Hornberger once more:
“Licencing is a special-interest legislation for the benefit of physicians and other medical personnel. Its primary purpose and effect are to limit entry into the medical profession in order to protect medical people from competition. Does licencing ensure competent doctors and nurses? If it does, then why do we continue to have so many malpractice judgments against doctors and other medical personnel? And one problem with licencing is that it seduces the public into believing that because a person has been licenced by the state, he must be competent. What would happen if licencing were repealed? Well, no one would run out into the street looking for a quack to perform heart surgery on him. […] What if someone needed a new doctor? The likelihood is the person would rely on the recommendation of his current physician. Moreover, well-established and well-known physicians in the community would band together to publish a list of recommended doctors in the area; private certifying agencies (i.e., Consumer Reports or Good Housekeeping) would do the same.” (Jacob Hornberger. The Dangers of Socialized Medicine. p. 22)
“the government pays for roughly half of all healthcare purchased in the US. Since Medicare and Medicaid patients pay little or nothing, it creates an incentive to consume more than one would value if they incurred the costs”
Medicare and Medicaid
What are the interventionist effects of Medicare and Medicaid? Aside from the extortion of resources, the two forms of medical welfare have negative effects on the demand-side of the equation.
The way it is affected is, the government pays for roughly half of all healthcare purchased in the US. Since Medicare and Medicaid patients pay little or nothing, it creates an incentive to consume more than one would value if they incurred the costs, which if the costs were internalised, it would create incentives to shop around for care. Up until the 1980s, Medicare and Medicaid reimbursed providers, meaning neither patient nor doctor had any incentive to keep either costs down. This lead to a sharp upward movement in prices for insurance and healthcare in general. As a result, many people and small businesses were and are, priced out of the insurance market.
The FDA, patents and insurance regulations also play a huge role in the high expense American’s pay for healthcare.
Insurance
Employer-Provided Health Insurance (1943) – While not mandatory in all states, Employer-Provided Health Insurance requires an employer to pay for the coverage of their employees. Since the individual patient is not facing the costs of said coverage, this leads to people not being as fiscally responsible as they would be; leading to higher risks and higher costs. This also plays a role in why low-pay workers find it hard to leave their job; if they did they would be at risk of not being covered should they face medical needs, leading to employees in states where it is mandatory being dependent on their employer.
Mandated Coverage – The state of California since 2011 has made it mandatory for insurance providers to cover maternity leave (legislation SB 299, AB 592, SB 222 and AB210) This means that even if a woman does not want children, or cannot have children for medical reasons; or because of age, she still has to pay for the coverage of something she will either never want, or never be able to have. This waste not only affects the insurer, but the policy holder, by forcing them to pay a higher price.
Mandatory Insurance – The Obamacare Individual Mandate, made it mandatory on the federal level for all American’s to purchase health insurance. This has the obvious effect of artificially forcing up the quantities being purchased and the demand, leading to higher prices for insurance and medical care. As of 2019 the mandate was no longer required on the federal level, however at least 5 states and the District of Columbia have maintained the mandate for purchasing health insurance.
FDA
Slow-Testing and Approval Process – The FDA’s process of approval times and testing has gone through a very regressive motion. Before 1962 the FDA was required to approve a drug within 180 days unless the new drug was proved to not be safe; meaning there was a time constraint on the FDA, and new drugs could get into the medical market faster. After 1962, said time constraint was removed, and since then the drug approval process has lengthened exponentially. To give a bit of context, prior to 1962 the time between filing and approval was an average of 7 months, after 1967 that time rose to 30 months, and by the late 1980s the time between filing and approval shot up to 8 – 10 years. This excessively lengthened process has seen the cost of testing new drugs rise to around $800 million per drug, and due to the lack of viable substitutes for patients has caused the price of drugs already on the market to rise.
Anti-Advertisement – Advertisement of approved drugs for newly discovered uses, which may be more beneficial than it’s conventional use, is prohibited under FDA rules. This leads to many companies not finding it worthwhile to re-evaluate an approved drug for alternative uses. This restriction has created a barrier to entry in the drug market; not only blocking entrepreneurial innovators from advertising their discoveries, in the attempt to alert consumers of what they may hold an absence of information over, but is designed to protect already existing drug companies from competition.
Patents
IP the Restrictor of Competition
IP is designed to protect the producer of a drug from competitors who wish to reverse engineer their drug, in order to sell similar drugs on the market. IP is not simply the protection of a brand, it restricts who can produce and sell what. It is IP which has led to the rising costs of epipens and insulin. An example of drugs without IP and drugs with, are painkillers and Epipens. In 2020 the average cost of a two-pack of Epipens was $699.82. Pain Relievers with no IP can be purchased at a low price of $3.88 for a 24 pack. If IP was removed from all drugs and reverse engineering by competitors was allowed, dominant drug companies would have to find new ways to innovate their drugs, lower their prices to withhold and stall competition, or be priced out of the drug market.
“Mandates and freedom are opposites. If a person is free, then that means he is not mandated to buy anything. If a person is mandated to buy something, then he is not free. Mandates are not a free-market alternative, because mandates violate free-market principles.” (Jacob Hornberger. The Dangers of Socialized Medicine. p. 14)
“Private doesn’t simply mean “for-profit”, private means there is no government intervention, micro-management, protections, controls or ownerships”
An Alternative to the NHS
Keeping in mind everything we’ve gone over, is it possible to have universal access to healthcare within a free market in healthcare? Yes; if you allow for variety in the means of acquiring medical care, and the ways to provide it.
What do I mean by this? Private doesn’t simply mean “for-profit”, private means there is no government intervention, micro-management, protections, controls or ownerships.
Assuming the reader understands how a for-profit provider would operate (like any other service provider), in order to save time we’ll simply look at what alternatives could exist alongside for-profit providers.
Limited Local Government Display
The British people are a very charitable people, and Britain has had a culture that values empathy and charity for centuries. The difficulty that comes with seeking help, is an absence of information, with regards to the existence of charities that can help people. Local councils can play a very limited role, in advertising all health-based charities that operate within their borough, or that operate nationwide, but which have easy access facilities within the borough. These advertisements could be in the form of notice boards in the council buildings, as well as mailing lists to communities the councils’ understand to have poor demographics.
This would not only expose large numbers of charities to potential donors who did not know these charities existed, but also to the poor who may not know where or who they can turn to.
To put my thoughts into actions, I recommend donating to BenendenHealth. They are a non-profit, affordable care provider that was established in 1905, with the purpose of joining people together to help with medical care when they need it. You can make a donation at https://www.benenden.co.uk/about-benenden/charitable-trust/donations/
Subscription Institutions
This one may seem a bit strange to the reader, so I’ll need to take some time to explain what I mean. The Subscription Institution proposal I’m making, is based on the structure and methods of provision of the Mises Institute. The Mises Institute is a non-profit organisation dedicated to spreading the economic theories of the Austrian School.
The Mises Institute, generates its funds via donations, but also raises funds through a subscription basis; where subscribers pay a monthly fee, and receive benefits such as discounts, newsletters, magazines, and updates on events for members. An additional means of raising funds is by selling products both to members and non-members. As of late, due to charitable donations the institute has begun its own Master Degree in Economics for a lower price than other universities; the average cost for a Masters course ranges from $20,000 – $60,000, whereas the Mises Institute charges around $4,000.
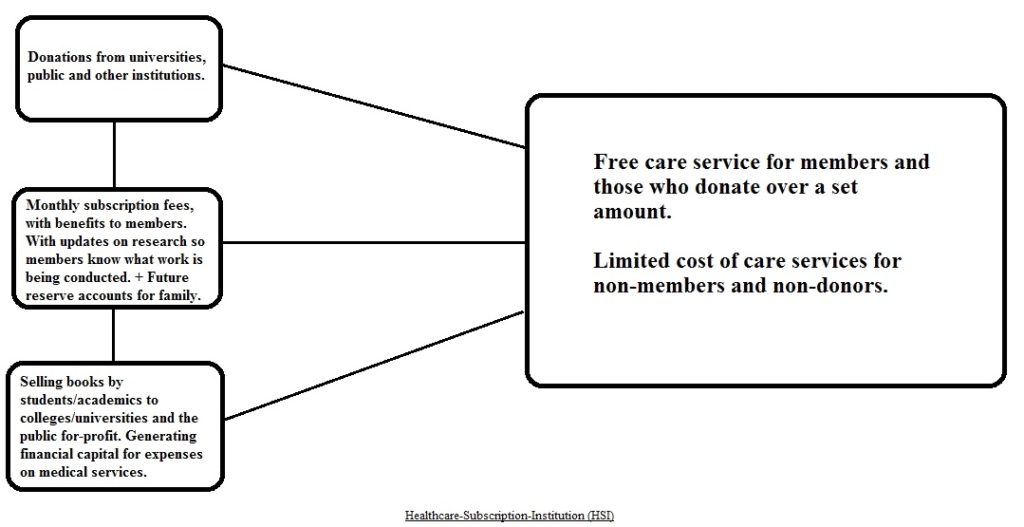
A similar format could be imagined for private, subscription-based healthcare institutions. We can refer to these as Healthcare-Subscription-Institutions (HSI).
Above we see a basic outline of how such an institution could function. They would receive donations from members of the public on a voluntary basis, as well as universities and other institutions who would mutually benefit from research being conducted.
Secondly, the option of a monthly subscription, would allow members of the public to receive certain benefits; such as free care services, newsletters on developments and research being conducted with/without collaboration with other institutions, and discounts on products such as books, human anatomy models, and health conferences.
Thirdly, the Healthcare-Subscription-Institution (HSI) would generate additional financial capital by selling books by academics, doctors and recently graduated students. This would benefit the producers of these books by expanding the access to their work, as well as assisting to build up a resume for recently graduated students.
Finally, Future-Reserve-Accounts would allow individuals to set up what could be likened to a savings account for their children or grandchildren. They would pay a monthly deposit, to which the HSI would use a fraction for further investments, branching out, diversifying their capital stock and creating additional research and services. At the payee’s end of life, the collected funds would be transferred to the declared recipient; either child or grandchild, with added interest.
This would result in a care service which would be free for members; due to continued commitment to their subscription payments, and a limited fee for non-members.
Healthcare in the UK is in desperate need of reform. We continue to not help our national situation by being in a state of denial and nostalgia for days and standards to which never even existed. One type of private healthcare would be as effective as a nationalised system; it cannot meet the demands of all. If universality is the principle which British people refuse to budge on, then a private system with a diverse way of providing care has a greater chance; allowing a wide variety of methods for providing care, would ensure a greater degree of people have access to care; we have a variety of methods for providing other products, so why not healthcare? Rather than an ultimatum between ‘for-profit or nothing’, or ‘nationalised or nothing’, let’s try a decentralised, denationalised variety of choice.
For-Profit, Non-Profit, Charities, One-to-One Personal Family Doctors, Healthcare-Subscription-Institutions; whichever you subjectively prefer, choice is the best cure for healthcare.
Sources:
Kristian Niemietz: Universal Healthcare Without the NHS (pp. 19-21)
Nick Hayes: English Historical Review (p. 659)
Kristian Niemietz: Universal Healthcare Without the NHS (pp. 24-25)